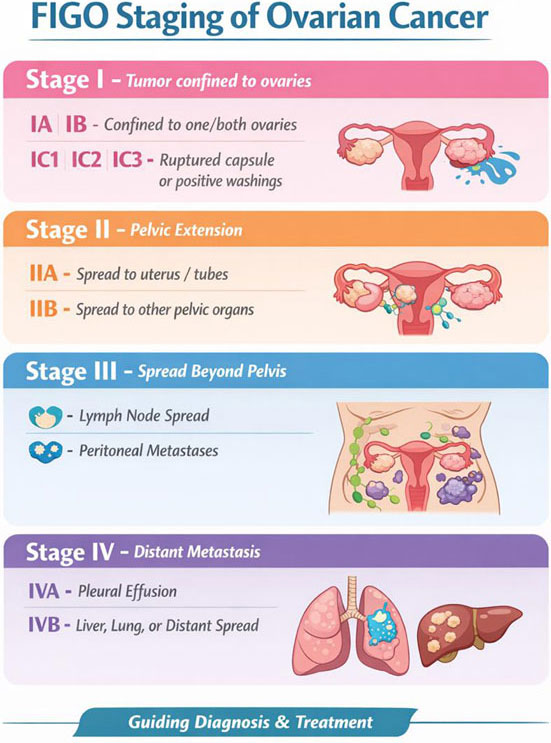
Ovarian cancer begins in the ovaries, which are responsible for producing eggs and female hormones. It occurs when abnormal cells grow uncontrollably and form a tumor, which may be solid or cystic.
Early detection is difficult because initial symptoms are mild or vague, which is why ovarian cancer is often called the “silent killer.” Only a small number of cases are diagnosed at an early stage.
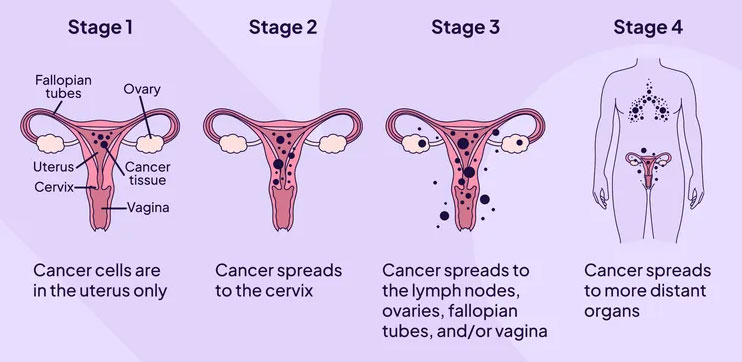
Ovarian cancer grows rapidly and can spread to the abdomen, lymph nodes, lungs, or liver if not treated on time.
Common warning symptoms include persistent bloating, pelvic or abdominal pain, feeling full quickly, loss of appetite, and frequent urination. Symptoms lasting more than two weeks should not be ignored.
Risk factors include increasing age, family history of breast or ovarian cancer, BRCA gene mutations, obesity, endometriosis, and prolonged hormone therapy.
Diagnosis involves pelvic examination, imaging tests like CT or MRI scans, and blood tests such as CA-125.
The main treatment includes cytoreductive (debulking) surgery followed by chemotherapy. Treatment by a gynecologic oncologist significantly improves outcomes.
Early detection combined with prompt treatment significantly improves treatment outcomes.

The uterus, also known as the womb, is the organ where a baby grows during pregnancy. Uterine cancer most commonly develops from the inner lining of the uterus, called the endometrium, and is therefore known as endometrial cancer.
One of the most important features of uterine cancer is that it often causes early warning signs, especially abnormal vaginal bleeding. Because of this, many women are diagnosed at an early stage, when treatment outcomes are usually very good.
There are two main types of uterine cancer. Endometrial adenocarcinoma is the most common and usually grows slowly. Uterine sarcoma is rare and develops from the muscle or supporting tissues of the uterus.
Common symptoms include bleeding after menopause, heavy or irregular periods, abnormal vaginal discharge, pelvic pain, or a feeling of heaviness in the lower abdomen.
Diagnosis is done through pelvic ultrasound and endometrial biopsy, which confirms the disease. Treatment depends on the stage and may include surgery, radiation, chemotherapy, or hormone therapy.
Finding the problem early and starting treatment on time leads to better recovery.
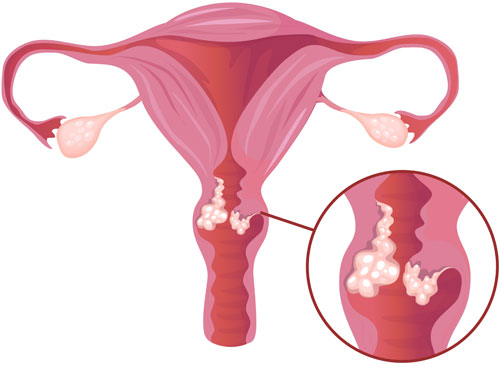
Cervical cancer is the fourth most common cancer among women worldwide, with around 660,000 new cases reported in 2022. Nearly 94% of related deaths occur in low- and middle-income countries due to limited access to vaccination, screening, and timely treatment.
Almost all cervical cancer cases are caused by persistent infection with high-risk types of Human Papillomavirus (HPV), a very common sexually transmitted infection. While most HPV infections clear naturally, long-term infection can lead to precancerous changes that may develop into cancer over 15–20 years.
Women living with HIV have a significantly higher risk and require earlier and more frequent screening.
Cervical cancer is highly preventable through HPV vaccination (recommended for girls aged 9–14 years) and regular cervical screening starting at age 30 (25 in women with HIV).
Early detection of precancerous changes allows simple and effective treatment, preventing cancer development.
If diagnosed early, cervical cancer is highly treatable with surgery, radiotherapy, or chemotherapy. Recognizing warning signs such as abnormal bleeding, unusual discharge, or persistent pelvic pain is crucial.
Awareness, vaccination, and regular screening remain the most powerful tools to eliminate cervical cancer.
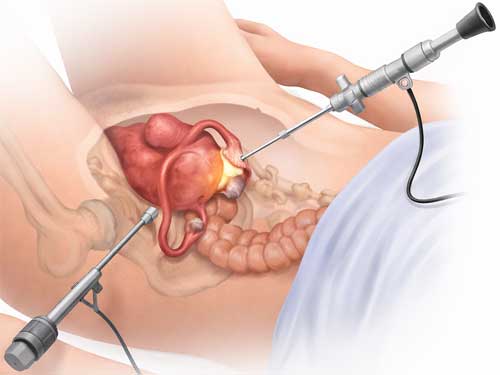
A hysterectomy is a surgical procedure to remove the uterus and can be safely performed using minimally invasive laparoscopic surgery.
There are different types of hysterectomy depending on the condition. A total hysterectomy removes the uterus and cervix while preserving the ovaries, so hormone levels remain unchanged in pre-menopausal women. A subtotal hysterectomy removes only the uterus and keeps the cervix, requiring future cervical screening. In some cases, the uterus, cervix, ovaries, and fallopian tubes are all removed, which can lead to menopause if done before menopause.
Hysterectomy can be performed through the vaginal, abdominal, or laparoscopic route. The laparoscopic method uses 3–4 small incisions and is a safe and effective alternative to open surgery when performed by trained surgeons, offering faster recovery and less pain.
The choice of surgical approach depends on the disease, uterine size, and the surgeon’s expertise.
Common reasons for hysterectomy include heavy menstrual bleeding, fibroids, endometriosis, adenomyosis, pelvic organ prolapse, and certain uterine or ovarian cancers.
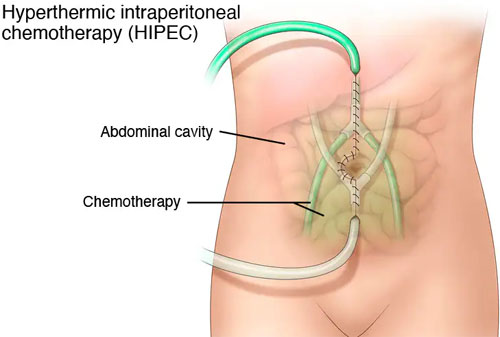
Advanced epithelial ovarian cancer is often diagnosed when the disease has already spread within the abdomen. The standard treatment includes cytoreductive (debulking) surgery followed by chemotherapy, where complete removal of visible disease is the most important factor for survival.
However, microscopic cancer cells may remain in the abdominal cavity even after successful surgery, leading to a high risk of recurrence.
HIPEC (Hyperthermic Intraperitoneal Chemotherapy) is a specialized treatment given immediately after surgery to destroy these remaining cancer cells. During HIPEC, heated chemotherapy is circulated inside the abdomen, allowing high drug concentration directly at the disease site with fewer systemic side effects.
Heat enhances the effectiveness of chemotherapy by improving drug penetration and increasing cancer cell destruction.
Scientific studies and clinical trials have shown that combining HIPEC with cytoreductive surgery improves recurrence-free and overall survival in selected patients with advanced ovarian cancer, without significantly increasing complications.
Quality of life may temporarily decrease after surgery but generally recovers and improves within a few months.

Vulvar cancer affects the external female genital organs, including the vaginal lips, clitoris, and surrounding skin. Most vulvar cancers are squamous cell carcinomas, which develop from the surface skin cells of the vulva. Less commonly, vulvar cancer may arise from gland-forming cells and is called adenocarcinoma.
Vulvar cancer usually develops slowly over many years and may begin as a precancerous condition known as Vulvar Intraepithelial Neoplasia (VIN). Early treatment of VIN can prevent progression to cancer.
Common symptoms include a lump or growth on the vulva, persistent itching or burning, skin color or texture changes, pain during urination, abnormal bleeding or discharge, non-healing ulcers, or wart-like growths.
Treatment of invasive vulvar cancer is mainly surgical. Surgical options include radical local excision, modified radical vulvectomy, or radical vulvectomy, depending on disease extent. Groin lymph node removal (lymphadenectomy) may also be required to assess cancer spread.
Right diagnosis at the right time leads to better results.

Vaginal cancer is a rare type of cancer that develops in the tissues of the vagina.
The vagina is a muscular canal that connects the cervix of the uterus to the outside of the body.It also serves as the birth canal during childbirth.This cancer usually grows slowly and is more common in older women.
Early detection improves treatment outcomes significantly.
The treatment of vaginal cancer is decided based on the stage, size, and exact location of the tumor. In early stages, surgery may be sufficient to remove the cancer completely. In more advanced cases, radiation therapy is commonly used, either alone or in combination with other treatments, to effectively control the disease and prevent its spread.

Gestational Trophoblastic Neoplasia (GTN) is a rare group of pregnancy-related tumors that develop from abnormal growth of placental (trophoblastic) tissue. It most commonly occurs after a molar pregnancy but can also develop following a miscarriage, ectopic pregnancy, or even a normal delivery.
GTN includes conditions such as invasive mole, choriocarcinoma, and placental site trophoblastic tumor. These tumors often produce high levels of the hormone beta-hCG, which helps in diagnosis and monitoring treatment response.
Common symptoms may include irregular or heavy vaginal bleeding after pregnancy, persistent high hCG levels, pelvic pain, enlarged uterus, or symptoms related to spread to lungs (such as cough or breathlessness).
Treatment depends on the type and stage of disease but is highly effective. Most cases respond very well to chemotherapy, and surgery may be required in selected situations. With early diagnosis and appropriate treatment, GTN has an excellent cure rate, even in advanced stages.
Early detection and regular follow-up ensure successful outcomes and preservation of future fertility in most patients.

Endometriosis is a chronic inflammatory disease in which tissue similar to the uterine lining grows outside the uterus, often causing pelvic pain, menstrual symptoms, and infertility.
Surgical treatment plays a central role and requires high precision, advanced expertise, and meticulous planning.
The primary goal of surgery is complete removal of the cancer along with all involved endometriotic tissue.
These surgeries are often complex due to dense adhesions, distorted anatomy, and involvement of nearby organs.
Structures such as the ovaries, uterus, bowel, bladder, or pelvic ligaments may be affected.
A thorough pre-operative evaluation using imaging and tumor markers is essential for surgical planning.
The procedure may involve radical excision, organ-preserving techniques, or multi-organ resection when required.
Precision is critical to ensure clear margins while protecting vital nerves, blood vessels, and organs.
Whenever feasible, minimally invasive approaches such as laparoscopy or robotic surgery are preferred.
These techniques offer better visualization, reduced blood loss, and faster recovery.
In advanced cases, surgery is often combined with chemotherapy or targeted therapy.
Management requires a multidisciplinary team approach for optimal outcomes.
Early diagnosis and expert surgical care significantly improve prognosis.
Post-surgical follow-up is essential to monitor recovery and prevent recurrence.
Individualized treatment planning ensures the best balance between disease control and quality of life.
Robotic surgery in gynecologic oncology is an advanced, minimally invasive technique used to treat cancers of the female reproductive system, including cervical, uterine (endometrial), and ovarian cancers. It utilizes a high-definition 3D camera and precision-controlled robotic instruments that allow the surgeon to perform complex procedures with greater accuracy and control.
This approach enables delicate dissection around vital organs, nerves, and blood vessels in the pelvis, which is especially important in cancer surgery. The robotic system enhances vision, flexibility, and stability compared to conventional laparoscopy.
Common procedures performed robotically include radical hysterectomy, total hysterectomy with lymph node dissection, staging surgery for ovarian cancer, and pelvic or para-aortic lymphadenectomy.
Benefits of robotic gynecologic cancer surgery may include smaller incisions, less blood loss, reduced post-operative pain, shorter hospital stay, faster recovery, and earlier return to daily activities.
Timely diagnosis and treatment with advanced surgical technology can significantly improve outcomes and quality of life for patients with gynecologic cancers.

Colposcopy is a simple diagnostic procedure used to closely examine the cervix, vagina, and vulva for abnormal or precancerous changes. It is usually recommended when a Pap smear is abnormal, HPV test is positive, or unusual bleeding or cervical changes are detected.
During the procedure, a special magnifying device called a colposcope is used to clearly visualize the tissues. If any suspicious area is identified, a small biopsy may be taken for laboratory testing. The procedure typically takes 10–20 minutes and is performed in an outpatient setting.
Colposcopy helps in early detection of cervical cancer, precancerous lesions, genital warts, cervicitis, and other abnormalities. Early diagnosis allows timely treatment and better outcomes.
Patients are advised to avoid intercourse, tampons, and vaginal medications 1–2 days before the procedure. Mild cramping or light spotting may occur afterward, especially if a biopsy is performed.
For expert colposcopy evaluation and women’s health care in Gurgaon, consult a qualified gynecologist for accurate diagnosis and appropriate management.
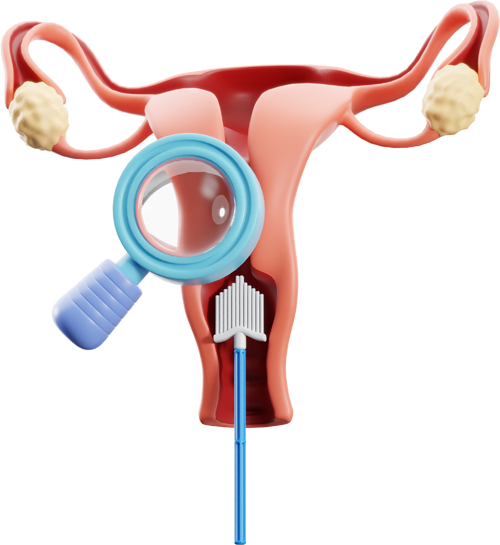
Cervical cancer screening is a preventive health check that helps detect abnormal or precancerous changes in the cervix before they develop into cancer. Regular screening plays a crucial role in early diagnosis and significantly reduces the risk of advanced cervical cancer.
The most common screening tests include the Pap smear and the HPV (Human Papillomavirus) test. These tests are simple, quick, and usually painless procedures performed in an outpatient setting.
Women are generally advised to start screening from the age of 21 and continue at regular intervals as recommended by their gynecologist. Early detection allows timely treatment and improves long-term outcomes.
Dr. Shalu provides comprehensive cervical cancer screening with a focus on early detection, patient comfort, and personalized preventive care. Regular screening is one of the most effective steps toward protecting women’s health.